
July 2025
Case Report: Keloidal Fibroma in a Dog
Author: Michaela C. Long, DVM
Co-author: Daniela Hernandez Muguiro, DVM, DACVP (Clinical Pathology); Brandon L. Plattner, DVM, PhD, DACVP (Anatomic Pathology)
Case Presentation
A three-year-old male castrated mixed breed dog presented with a 1x2cm mass on the lateral surface of the right proximal hind limb that had been present for two months. A fine needle aspirate of the mass was initially submitted for cytologic evaluation, and one month later an excisional cutaneous biopsy was submitted for histologic evaluation. No changes in the mass had been noted since the submission of the initial fine needle aspirate.
Cytology
One pre-stained (Diff-Quik) slide was examined and showed a highly cellular population of spindle to occasionally stellate cells (Figures 1 and 2). Individual and aggregates of cells were often associated with extracellular eosinophilic matrix ranging from fibrillar to glassy in appearance, consistent with hyalinized collagen. The cells showed moderate to abundant amounts of mid-blue cytoplasm with tapered ends. The cells had ovoid to rarely round nuclei with finely stippled chromatin and one to three small nucleoli. There was mild to moderate anisocytosis and anisokaryosis. No mitotic figures were seen. There were rare well granulated mast cells scattered throughout.
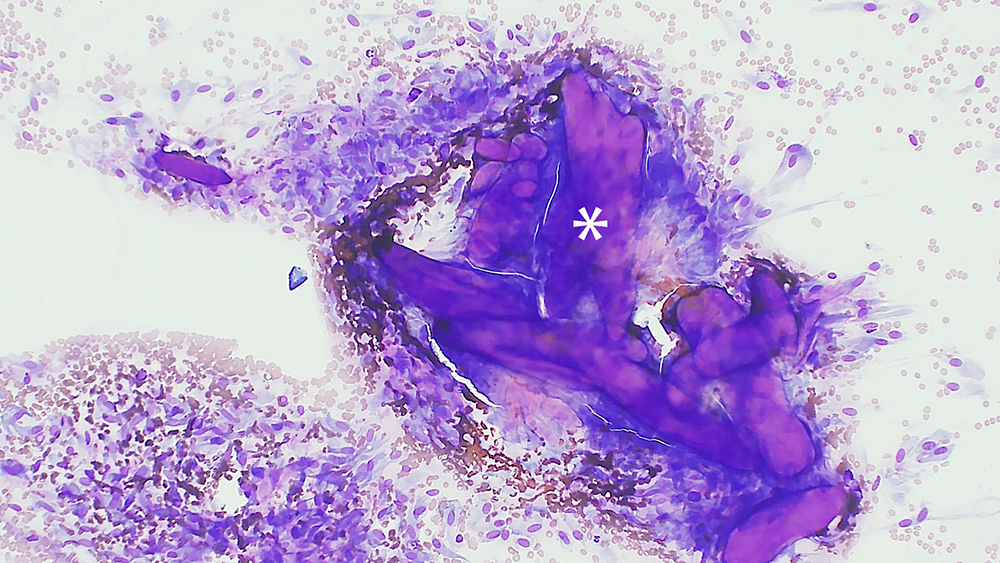
Figure 1: Fine needle aspirate of a subcutaneous keloidal fibroma from a 3-year-old male castrated dog. Hyalinized collagen surrounded by neoplastic spindle to stellate cells. Diff-Quik, 100x magnification.
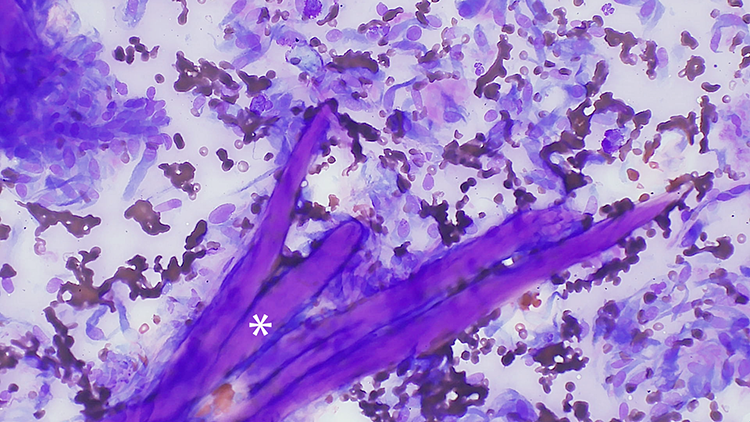
Figure 2: Fine needle aspirate of a subcutaneous keloidal fibroma from a 3-year-old male castrated dog. Higher magnification view of the hyalinized collagen surrounded by neoplastic spindle to stellate cells. Diff-Quik, 200x magnification.
Histopathology
Three slides containing the excised mass were examined (Figures 3 and 4). Expanding the subcutis and elevating the dermis and epidermis was a densely cellular, well demarcated, expansile, unencapsulated nodular neoplasm. Neoplastic cells were arranged in bundles and streams supported by a dense fibrovascular to collagenous stroma; importantly, there were many haphazardly arranged thick eosinophilic homogenous hyalinized collagen fibers. Neoplastic spindle cells had indistinct cell borders, moderate amounts of lightly eosinophilic cytoplasm, a single ovoid nucleus and finely stippled chromatin with occasional nucleoli. There was mild pleomorphism of the cells, and a low mitotic count (2 observed per 2.37mm2). There was minimal inflammation and no evidence of necrosis. The surgical margins were wide, with normal fat completely surrounding the mass.
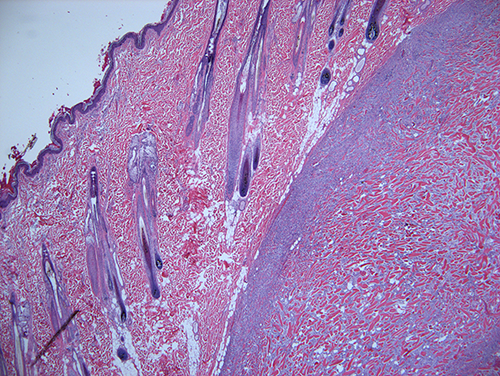
Figure 3: Histologic section of a subcutaneous keloidal fibroma from a 3-year-old male castrated dog. A well demarcated, unencapsulated spindle cell neoplasm elevates the dermis and epidermis. H&E 20x magnification.
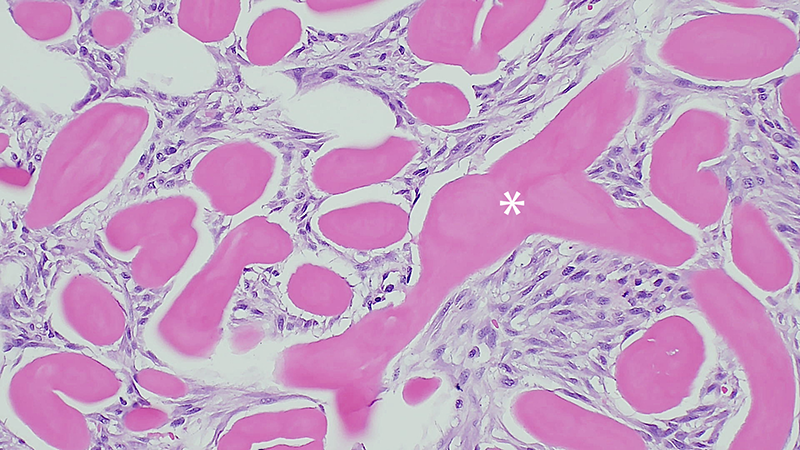
Figure 4: Histologic section of a subcutaneous keloidal fibroma from a 3-year-old male castrated dog. Neoplastic fibroblasts surround numerous large fibrils and bundles of hyalinized eosinophilic collagen. H&E 200x magnification
Final Diagnosis
The cytologic diagnosis was mesenchymal neoplasia, most consistent with a keloidal fibroma/fibrosarcoma, due to the many spindle cells intermixed with prominent eosinophilic hyalinized collagen; the diagnosis was confirmed as keloidal fibroma by histopathologic examination.
Case Discussion
Mesenchymal neoplasms arise from the various supportive structures in skin and subcutaneous tissues, including fibrous connective tissue, smooth muscle, blood vessels, lymphatics, fat, or nerves.1 Fibromas are a specific benign mesenchymal tumor that arise from fibroblasts in connective tissue.1, 4
Keloidal fibromas/fibrosarcomas are a subset of fibromas/fibrosarcomas that are differentiated by the abundant eosinophilic hyalinized collagen fibrils within the neoplasm that are not produced by other subtypes.1, 2, 4 Keloidal fibromas are benign, collagen-rich, well circumscribed or encapsulated lesions found in the skin of dogs.1, 3, 4 These tumors are rare, but can occur in dogs of any age or breed, with a predisposition for males.1 Common locations include the dermis or subcutaneous tissue of the flank, thorax, or shoulder.1
Cytologically, it may be difficult to differentiate between keloidal fibroma and keloidal fibrosarcoma as criteria of malignancy such as the degree of anisocytosis and anisocytosis overlap. The terms keloidal fibroma and keloidal fibrosarcoma are often used interchangeably.1, 2, 3, 4 Therefore, the final diagnosis should rely on the histopathologic features of the lesion. fibroma is the correct terminology when the histomorphologic features of malignancy are not observed. Malignancy (i.e., fibrosarcoma) should be considered if there is an increase of cellular density, mitotic activity, nuclear or cellular pleomorphism, infiltrative growth pattern, or metastasis, which are all described for other soft tissue neoplasms.1 Complete and wide excision of keloidal fibroma is normally curative.1, 3, 4
Canine keloidal fibromas or fibrosarcomas should not be confused with the so-called keloids in humans. Keloids are associated with previous trauma and differ in the amount of hyalinized collagen present, being more prominent in canine keloidal lesions. While not always present in keloids, hyalinized collagen is the diagnostic feature of canine keloidal lesions.5 .2
References
- Hendrick MJ. Mesenchymal tumors of the skin and soft tissues. Tumors in Domestic Animals. 5th Meuten DJ editor. 2017. Pages 142-144.
- Mikaelian I, Gross TL. Keloidal Fibromas and Fibrosarcomas in the Dog. Veterinary Pathology. 2002;39(1):149-153. doi:10.1354/vp.39-1-149
- Palić J, Saey V, van der Lugt J, Baumgärtner W, Hülskötter K. Cytologic, histopathologic, and immunohistochemical features of keloidal fibroma in a dog. Vet Clin Pathol. 2023 Dec;52(4):676-680. doi: 10.1111/vcp.13282. Epub 2023 Sep 3. PMID: 37661191.
- Roccabianca P, et al. Fibroma. In: Surgical Pathology of Tumors of Domestic Animals, Ed. By M Volume 3: Tumors of soft tissue (1.1.1), pages 80-84,103.
- Lee JY, Yang CC, Chao SC, Wong TW. Histopathological differential diagnosis of keloid and hypertrophic scar. Am J Dermatopathol. 2004 Oct;26(5):379-84. doi: 10.1097/00000372-200410000-00006. PMID: 15365369.