
March 2019
Rheumatoid Factor (RF) and Anti-nuclear Antibody (ANA)in the Diagnosis of Autoimmune Disorders in Veterinary Patients
By Drs. Brandy Kastl and Nora Springer
The diagnosis of autoimmune disorders in veterinary medicine can be challenging. Serum auto- antibody titers, particularly for rheumatoid factor (RF) and/or anti-nuclear antibody (ANA), are often employed when autoimmune disease is suspected. However, both of these tests are of greatest diagnostic utility when interpreted in context of the complete clinical picture. Understanding both the strengths and pitfalls of autoantibody detection will improve accurate interpretation of positive results. For this article,we will be using the diagnostic work-up for polyarthritis as an example of the clinical utility of both RF and ANA.
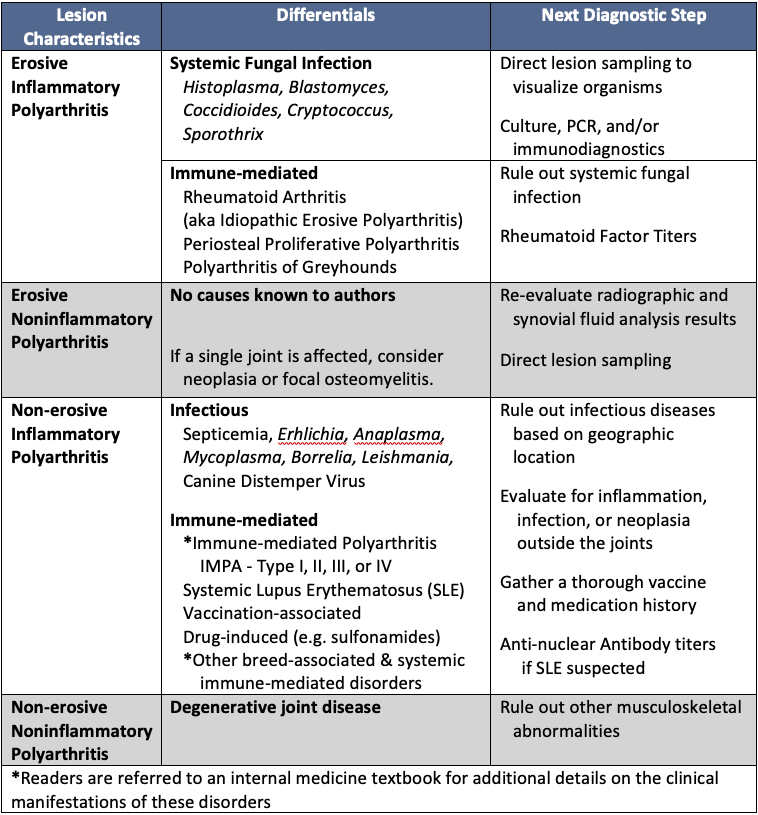
Serum RF and ANA titers are often utilized in the diagnostic work-up for suspected immune-mediated polyarthritis in dogs (see Table 1 – Diagnostic Approach to Canine Polyarthritis). Diagnostic evaluation of polyarthritis, regardless of species,should first begin with radiographs of the affected joint(s) and concurrent synovial fluid analysis. Radiographs determine if arthritic lesions are erosive (i.e. bone involvement) or nonerosive (i.e. no bone involvement). Meanwhile, synovial fluid analysis identifies inflammation and, on occasion, infectious organisms. An absence of microscopically visible organisms within synovial fluid does not exclude an infectious etiology; thus, appropriate infectious disease testing is needed. Ultimately, the combination of radiographic lesion characteristics, synovial fluid findings, and ancillary infectious disease test results will narrow the differential list (see Table 1) in caninepolyarthritis. When lesion characteristics fit and infectious diseases have been excluded, both RF and ANA titers provide additional support for a diagnosis of rheumatoid arthritis (RA) or systemic lupus erythematosus (SLE), respectively.
 |
|
Figure 1: Rheumatoid Factor Schematic |
Rheumatoid arthritis should be considered in cases of erosive, neutrophilic polyarthritis with no identifiable infectious etiology. Additional information on the diagnosis of RA, can be found at www.rheumatology.org within the 2010 ACR-EULAR Classification Criteria for Rheumatoid Arthritis which is considered applicable for veterinary species. In RA, autoantibodies directed against the fragment crystallizable (Fc) region of IgG antibodies accumulate (Figure 1). These IgM,IgA, or IgG autoantibodies are collectively referred to as rheumatoid factor (RF). Under normal circumstances, RF facilitates the removal of antibody-antigen complexes following an immunologic response. Because of this normal immunologic function, increased serum RF titers are not pathognomonic for RA and may be present in a small percentage of normal individuals or those with other chronic inflammatory conditions. In patients with RA, excessive RF production occurs after the initial onset of joint inflammation and subsequently potentiates arthritis formation via immune complex deposition within joint tissues. Due to this delay in RF accumulation, a small percentage of patients with RA will have negative RF titers. Regardless, determining serum RF titers remains a mainstay in the diagnosis of RA.
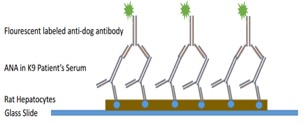
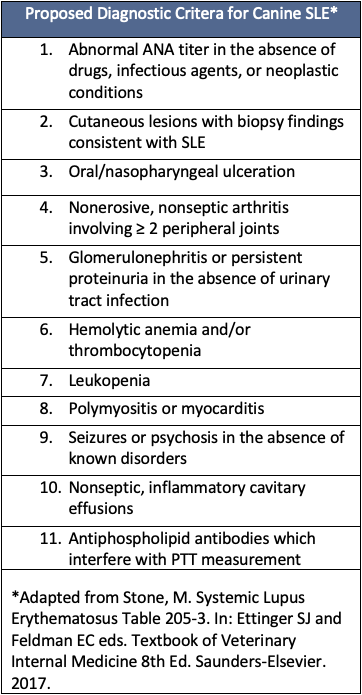
In contrast to RA, systemic lupus erythematosus (SLE) causes a non-erosive, inflammatory polyarthritis. In dogs, a diagnosis of SLE is often based on the presence of ≥ 2 clinical signs associated with autoimmunity(Table 2. Proposed Diagnostic Criteria for Canine SLE) in combination with a serum ANA titer > 1:160. Antinuclear antibody (ANA) is an umbrella term for autoantibodies directed against various nuclear antigens, such as histones and DNA. As with RF, a positive serum ANA titer is not pathognomonic for a diagnosis of SLE. Positive ANA titers may be observed in healthy individuals or associated with chronic inflammation (e.g. atopic dermatitis, Doberman hepatitis), infectious diseases (e.g. Ehrlichiosis, Leishmaniasis), neoplasia, or medications (e.g. sulfonamides, penicillin, tetracyclines). Thus, detection of serum ANA should be reserved for clinical cases in which SLE is strongly suspected. Because nuclear antigens are well-conserved between mammalian species, canine ANA titers at KSVDL are determined via indirect flourescent antibody detection utilizing rat hepatocytes as a substrate (Figure 2). Multiple serial dilutions of the patient’s serum are incubated with a thin preparation of rat liver cells. ANA present within the serum binds to the nuclei of the rat hepatocytes. Next, a secondary flourescent-labeled antibody is added to highlight the patient’s antibodies (i.e. ANA’s) complexed with their nuclear antigens (Figure 2).
|
|
|
|
Figure 2A. Schematic of Indirect Flourescent Antibody Detection of Canine Serum ANA Titers (Not drawn to scale). |
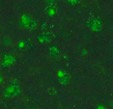
Figure 2B. Positive test result with immunofluorescence localized to nuclei. |
In conclusion, serum RF and ANA titers can be useful in the diagnosis of autoimmune disorders. Importantly, both serum RF and ANA titers should be reserved for patients with clinical symptoms compatible with rheumatoid arthritis and systemic lupus erythematosus, respectively. Infectious diseases, other autoimmune disorders, and neoplastic conditions should be effectively ruled out prior to performing these tests and especially before interpreting positive results. The KSVDL Clinical Immunology Laboratory currently offers validated commercial detection of serum RF and ANA titers for canines. Approximately 1-3 mL of serum, separated from the blood clot and placed within a fresh red top tube, are requested for testing. Once separated, serum should be stored in the refrigerator and shipped with a cold pack within 1-2 days of collection. For additional questions regarding either of these tests, please contact KSVDL Client Care at 1-866-512-5650 or 785-532-5650.
|
Table 1. Diagnostic Approach to Canine Polyarthritis |
Table 2: Proposed Diagnostic Criteria for Canine SLE |
 |
 |
NEXT: Watch for the Long-horned Tick This Season
Return to Index