
May 2019
A Case of Erythema Multiforme in an 11-month-old Pembroke Welsh Corgi: A Case Study
By Drs. Dina Steineker*, Jonathon Sago, Mary Bagladi-Swanson** and Charan Ganta
* Animal Health Center of Wichita, Kansas
** Veterinary Health Center, College of Veterinary Medicine, Manhattan, Kansas
Kansas State Veterinary Diagnostic Laboratory, College of Veterinary Medicine, Manhattan, Kansas
Clinical History
At a routine puppy examination in September 2018 (DOB: 06/15/2018), the owner reported that the patient was chewing at his leg. A suspicion of environmental allergies was present. Examination at that time revealed saliva staining and wetness on the left rear limb and dark, waxy debris in the external ear canals. Cytology of the ears revealed Malassezia, thus the ears were cleaned and treated for otitis externa. Three weeks after the initial visit, the owner reported that the patient had stopped chewing at his leg. At both visits DA2PP vaccines and pyrantel were administered, and Trifexis® was sent home for monthly administration.
|
|

The patient was again presented to Animal Health Center of Wichita, Kansas in April 2019 with facial pruritis, papules located at the lateral canthi of both eyes and the scrotum, and moist dermatitis on the left lateral trunk and hip (Figure-Before). The affected regions were clipped and flushed with chlorhexidine and a subcutaneous injection of 80 mg of Convenia® was administered. Malacetic-Wet-Wipes® were sent home at time of discharge. Approximately 14 days later, the condition had progressed to thick scabs at the lateral canthi and scrotum with new lesions on the dorsal muzzle, pinnae, and plantar surface of the metatarsals (Fig-Before). A skin scraping was negative for parasites.
Laboratory Testing
Multiple 6 mm skin biopsy sections from different areas of the skin were submitted for histopathological analysis.
|
|
| Figure A and B Histopathology |
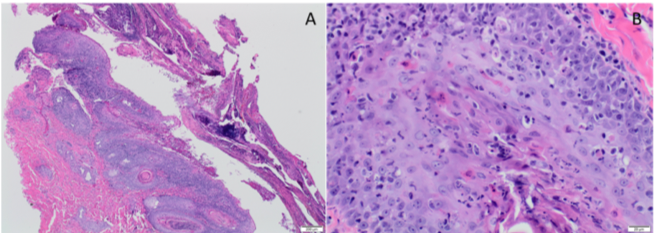
The microscopic lesions were consistent with Erythema Multiforme (EM) with likely secondary pyoderma. All the biopsies submitted had similar lesions on microscopic examination from multiple locations. The epidermis was hyperplastic with multifocal erosion and ulceration with marked crusting and cell debris. (Figure A) Both the epidermal and follicular epithelium had multifocal apoptosis of keratinocytes at multiple levels of epidermal layers along with lymphocytic infiltration in the epidermis. There were areas of interface dermatitis with predominantly lymphocytic infiltration. (Figure B)
Treatment
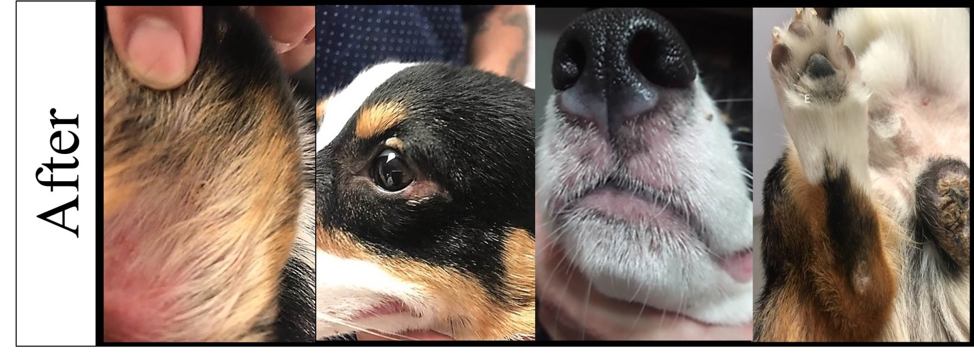
Following clinical and histopathological diagnosis of EM, a treatment plan was initiated upon consultation with Dr. Bagladi, a clinical professor of dermatology at Veterinary Health Center, College of Veterinary Medicine. The treatment included prednisolone at 2 mg/kg BID and terbinafine at 30 mg/kg SID. After seven days of therapy, significant clinical improvement was reported with resolution of pruritus and decreases in the size of alopecic and erythematous regions in all affected areas with crusts falling-off (Figure-After). Prednisolone was then tapered to SID dosing with a recommended recheck in seven days.
|
|
Summary
The histopathological lesions presented in this case are considered typical for EM. The clinical and gross pathological presentation of numerous skin lesions often overlap, hence histopathological analysis is often recommended to narrow down the list of differentials. The etiology however remains unknown in this case, previous reports have indicated the Pembroke Welsh Corgi as one of the breeds that are predisposed to this condition.
Reported Causes of Erythema Multiforme in Dogs
Erythema multiforme is a cutaneous reaction pattern of multifactorial etiology reported in dogs, cats, horses, cows, and ferrets. The most commonly involved sites in dogs include the ventrum, mucocutaneous junctions, oral cavity, pinnae, and footpads. The pathophysiology of EM is proposed to be a host-specific T-cell mediated hypersensitivity. The cellular immune response is directed against various keratinocyte-associated antigens, including those associated with drugs, infections (viral, fungal, and bacterial), neoplasia, various chemicals, foods, and connective tissue diseases. CD8+ T lymphocytes bind to antigenically altered keratinocytes and trigger apoptosis of keratinocytes/squamous epithelial cells.
| Infectious Diseases |
Drugs Implicated |
Neoplasia | Miscellaneous Causes |
|
|
|
|
|
|
Acknowledgements
The images are courtesy of Dr. Dina Steineker, DVM, Animal Health Center of Wichita, KS